
Zika
Zika fever is a typically imported disease and is not endemic in our country. However, it can give rise to native cases thanks to the spread of one of its vectors, the Asian tiger mosquito. Symptoms are similar to that of a mild influenza.
CAUSATIVE AGENT AND INFECTIVE CYCLE
Zika fever and its complications are caused by the Zika virus, which carries the same name (ZIKV). It is a Flavivirus that is closely related to those that cause dengue, yellow fever, West Nile, and Japanese encephalitis.
ZIKV is primarily transmitted with an infected mosquito bite. It has been isolated from the Aedes aegypti (also known as the yellow fever mosquito), and the Aedes albopictus (better known as the Asian tiger mosquito which is also widespread in Italy). Recent laboratory studies have demonstrated that both mosquitoes are competent in the amplification and transmission of the ZIKV virus.
Other mosquito species belonging to the Aedes genus (in particular, Ae. africanus, Ae. polynesiensis, Ae. unilineatus, Ae. vittatus and Ae. hensilli) are considered potential vectors of ZIKV according to some published studies.
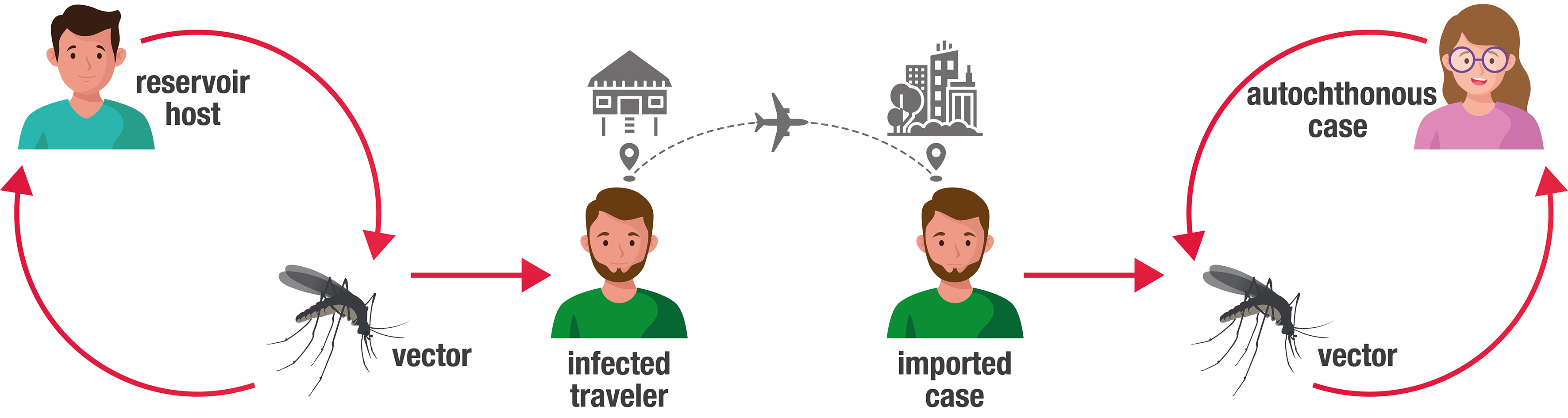
The original host is not known, but it is reasonable to assume that it was a monkey. In countries where the disease is endemic, the reservoir is man. There are two main strains, one African, and one Asian that has also recently emerged in the Pacific and the Americas.
There have also been additional ways of transmission:
- congenital or intrauterine transmission that occurs when a woman contracts ZIKV infection during pregnancy before childbirth, and the virus passes to the fetus (a study has shown that the host’s immune system can contribute to the pathogenesis of microcephaly; ZIKV is highly neurotropic and can therefore interfere with fetal development either directly, infecting the brain, or indirectly, infecting the placenta);
- perinatal transmission occurs when a woman contracts the ZIKV infection within approximately two weeks of childbirth and the virus passes to the new-born at or around the time of childbirth;
- sexual transmission;
- accidental contagion transmission during laboratory activities (rare cases);
- there is also a potential risk of ZIKV transmission through blood transfusions, hemopoietic stem cell transplantation, sperm donation, and organ transplantation.
ZIKV has been detected in the blood, urine, amniotic fluid, semen, saliva, and body fluids present in the brain and in the cerebrospinal fluid (CSF) of infected people.
SYMPTOMS AND COURSE OF THE DISEASE
In 80% of cases, the infection is asymptomatic. However, when symptoms do occur, they include: a rather modest febrile state (38,5°C), transient joint pain with possible swelling of the joints (mainly in the hands and feet), maculopapular skin rash - which often starts from the face, redness of the eyes, or non-purulent bilateral conjunctivitis; as well as several non-specific general symptoms, such as myalgia, asthenia, and headaches.
The incubation period has not yet been clarified but is likely to vary between 3 and 14 days after having been bitten by an infected mosquito. Symptoms of the pathology are generally mild, and the disease is usually characterized by a short-lived, self-limiting febrile disease that can last 2 to 7 days, without serious complications and with a low rate of hospitalization. The disease may be mistaken for dengue.
ZIKV can only be lethal in these rare cases: with people with pre-existing chronic diseases and severely immunosuppressed subjects.
On March 10th, 2017 (the last issued periodic report by the WHO with regards to the situation in the world), microcephaly and other malformations of the central nervous system, which are potentially associated with the ZIKV infection, or indicative of congenital infection, were reported in 31 countries, or territories; 23 countries or territories reported an increase in the incidence of Guillain Barré syndrome (SGB), and/or laboratory confirmation of ZIKV cases among SGB cases. Current research does show scientific consensus that ZIKV is a cause of microcephaly and Guillain Barré syndrome.
It has been reported that congenital ZIKV infection may be associated with a wide range of brain abnormalities, including microcephaly, craniofacial disproportion, intracranial calcifications, atrophy, and brain asymmetry, abnormal or absent brain structure, hydrocephalus, and neuron migration disorders.
The following neurological problems have also been reported: hypertonia, spasticity, hyperreflexia, irritability, tremors, seizures, dysfunctions of the brain stem, contracting of the limbs and dysphagia.
As for the eye, the following problems have been reported: microphthalmia, crystalline lens subluxation, cataracts, intraocular calcifications, optic nerve atrophy, optic nerve hypoplasia, macular degeneration, macular chorioretinitis, chorioretinal atrophy.
Other anomalies that have been reported include excessive and redundant scalp, arthrogryposis, and clubfoot.
However, there are other possible causes of congenital microcephaly, which include genetic disorders (chromosomal abnormalities), craniosynostosis, cerebral anoxia, alcohol consumption, mercury, radiation, and severe malnutrition in pregnancy. In addition, there are other maternal infections that can cause microcephaly which include cytomegalovirus, herpes simplex, rubella, lymphocytic choriomeningitis, chicken pox, syphilis, and toxoplasmosis.
TREATMENT AND PREVENTION
There is currently no vaccine to prevent ZIKV infection, nor is there any specific treatment for ZIKV infection or associated diseases. The therapy is symptomatic and is mainly focused on a pain relieving, antipyretic, and antihistamine therapy to reduce itching caused by a skin rash. In addition, bed rest and fluid replenishment are recommended.
The only way to prevent infection is to avoid being bitten by infested mosquitoes. Travelers or residents in an endemic country can take preventative measures when there is ongoing transmission.
Taking appropriate measures is essential:
- covering exposed skin with appropriate clothing (long sleeves and long trousers) during the times of day when the vector mosquito is most active (from sunrise to sunset);
- use repellents;
- ensure physical barriers are in place (mosquito nets on doors and windows);
- spend nights in places protected by mosquito nets.
In 2019, WHO updated their guidelines to prevent the sexual transmission of the Zika virus. It reduced the recommended period of having protected sex or practicing sexual abstinence from six to three months for men, and two months for women.
Last modified: Mar 2021
")
")